Dewinter G, Staelens W, Veef E et al.
British Journal of Anaesthesia 2018: 120 (1): 156-163.
Question
Would a simplified algorithm for PONV prophylaxis reduce the incidence of PONV in adult patients undergoing elective non-cardiac non-day-case surgery under general anaesthesia?
Study design
Quasi-experimental design
Single-centre, before and after study
2 x 5-working day audits (excl. Sat/Sun)
Initial audit using original algorithm Jan 12-18, 2016
Follow-up audit using simplified algorithm Nov 28 – Dec 2, 2016
University Hospitals Leuven, Belgium
Adult patients (Audit 1: 257 screened, 46 included, n=211. Audit 2: 231 screened, 30 excluded, n = 201) undergoing general anaesthesia
Inclusion criteria:
All adult patients >18 years old
Admitted to our post-anaesthesia care unit (PACU)
Undergoing elective, non-cardiac, non-day-case surgery, under general anaesthesia
Exclusion criteria:
Emergency procedures
Admitted to ICU/HDU
Patients expected to require overnight ventilation
Statistics
Fisher’s exact and Manne Whitney U tests were used to compare groups
Uni and multivariable logistic-regression models with a binomial logit link function were used for all binary outcomes
Poisson regression was used for count data
Primary outcome a p-value of 0.025
24 h PONV incidence, the multivariable logistic regression was risk adjusted
Logistic-regression analyses, the 10% and 20% Apfel risk strata were combined
Interventions
Initial algorithm
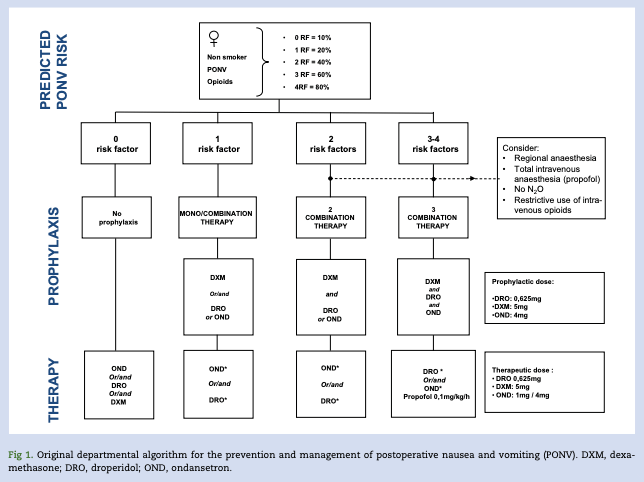
Simplified algorithm

Primary outcome
PONV incidence 1h and 24 h post-op
Secondary outcomes
- Incidence of PON & POV
- Accurate Apfel score
- Compliance with guidelines
- Anti-emetics administered
- Use of a rescue medication
Results
211 (1st) v 201 (2nd)
Primary outcome
Reduction in PONV over 24h (33% (69/211) vs 22% (45/201) P=0.02) RRR 33%, ARR 11%
Statistically significant when controlling for different confounders
Secondary outcomes
- No difference in PON & POV over 1h or POV over 24h
- Apfel score predicts PONV risk
- But was poorly calculated (correct in 36% v 42%)
- Simplified algorithm improved compliance with guidelines from 18% to 46%
- Use of rescue medication reduced during 2nd audit
- 58 pts (102 anti-emetics doses) v 30 (61), P=0.002
Discussion
- Low adherence to PONV guidelines is a well-known problem
- Uncertain how best to improve compliance with guidelines
- Electronic prompts/reminders rely on accurate calculation of risk – which was demonstrably poorly done – and have been shown not to work
- Simplification is effective
- Some patients will be over-treated but risk of harm is low
Strengths
- Relevant question
- PONV an issue
- Non-compliance with guidance is recognised issue
- Sample reflective of KH
- Reflective of KH practice
- Similar drugs, similar groups
- Well matched groups with bias minimised by lack of awareness of audit
- Significant difference in PONV rates over 24h
Limitations
Stated
- Short observation periods
- Study sample might not reflect the population incidence
- Clinical guidelines are introduced by means of a lecture given to the residents in their preparation year; the first audit occurred 5 months, and the second audit occurred 4 months, after their commencement.
- Poor calculation of PONV risk may have caused “non-compliance”
- Correct calculation and knowledge/reminder of guidelines may have improved performance
- Unclear cause of the reduction of the PONV incidence
- Introduction of the simplified algorithm
- Improved compliance with algorithm
- Increased number of anti-emetics given
Not-stated
- The beta-error (power) of the study is not specified
- No data on ethnicity – ?generalisable
- Majority of patients non-smokers and planned post-op opioid use
- No mention of N2O
- Significant number given no antiemetic (35% in initial audit)
- No mention of cost analysis or SEs of anti-emetics
- Un-blinded study with no control group
- Risk of Reporting validity – measurement method/accuracy changed between audits
- Risk of Regression-to-the-mean – particularly good or bad weeks
- Risk that audit itself improved awareness and improved performance
- Risk that introduction of novel guidelines (irrespective of content) improved awareness and improved performance
Study conclusions
The introduction of a radically simplified and mainly sex-centred PONV algorithm for the prophylaxis of PONV resulted in a significant reduction of PONV incidence and in a better compliance with the institutional algorithm.
Summary by Dr A Feben. Journal Club Meeting 27 June 2019.
