Gagey A-C, de Queiroz Siqueira M, Monard C et al.
Anaesthesia 2018, 73, 304-312
Aim of Study
Does qualitative ultrasound assessment of gastric contents lead to an appropriate change in the management of general anaesthesia planned according to clinical assessment in non-elective paediatric surgery.
Design and Location
Single centre prospective observational cohort study in paediatric hospital (France).
Methodology
Inclusion criteria:
– Children aged 2months-16yrs undergoing urgent or emergency surgery under GA
– Parental consent
– No contraindication to NG tube
Method
1) Routine pre-operative assessment by anaesthetist who classified ‘presumed gastric contents’ based on history as: ‘no contents’, ‘contents present’ or ‘cannot conclude with confidence’.
Anaesthetic makes a plan for induction of either RSI or routine induction.
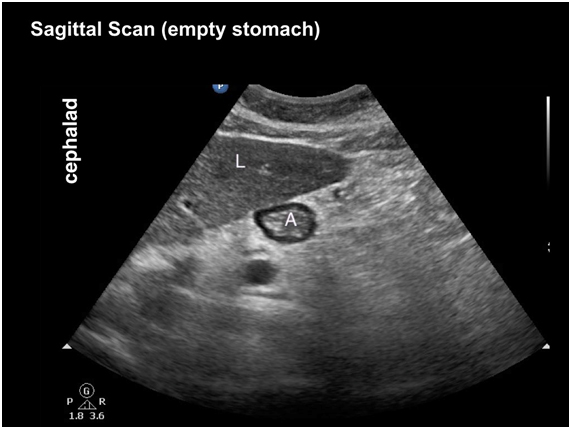
2) Ultrasound assessment by an operator (blinded) to qualitatively assessed in semi-recumbent and right lateral decubitus positions as ‘empty stomach’ or ‘contents present’.
3) Anaesthetist given results of ultrasound and given opportunity to revise induction plan.
4) Multi-port NG tube inserted post induction & gastric contents aspirated by a nurse (blinded). Stomach contents classified as ‘below risk threshold’ or ‘above risk threshold’ if: clear fluid > 0.8ml/kg, thick fluid or solid particles.
Primary Outcome
Qualitative ultrasound assessment of gastric contents leads to appropriate change in the management of general anaesthesia planned according to clinical assessment.
Secondary Outcome
Qualitative ultrasound assessment of gastric contents accurately diagnoses gastric fluid content > 0.8 ml/kg.
Statistics
Data were tested for normality of distribution using Shapiro–Wilk’s W-test.
Incidence data were compared using Fisher’s exact test or chi squared as appropriate (p < 0.05 was considered as statistically significant)
Sensitivity, specificity, negative and positive predictive values of conclusive ultrasound examinations to identify stomach contents above the risk threshold were calculated with 95%CI, using the Wilson method with continuity correction.
Results
144 children were recruited.
The anaesthetic induction plan changed in 67 (47%) children after ultrasound examination of the antrum was performed.
The rate of appropriate anaesthetic induction technique according to actual gastric contents was significantly improved after ultrasound examination of the antrum vs. after clinical assessment, 121 of 143 (85%) vs. 70 of 143 (49%; p < 0.00001).
Qualitative ultrasound assessment of gastric contents was not conclusive in 13 (9%) children, because of inadequate images (7), gas in the stomach (4) and anxiety and agitation (2).
Definitive ultrasound examination of the antrum allowed diagnosis of stomach contents above the risk threshold with a sensitivity (95%CI) of 94% (84–98%), specificity of 83% (71–91%), negative predictive value of 93% (82–98%) and a positive predictive value of 85% (74–92%).
Conclusions/Discussions
Pre-operative clinical assessment for the risk of pulmonary aspiration of gastric contents is inaccurate, since this led to an inappropriate anaesthetic induction plan in more than half of patients.
Qualitative ultrasound assessment can be used to accurately predict stomach contents above and below a risk threshold. The alternative method is quantitative cross sectional area methods.
Stated Limitations from the Study
Single centre study, only 3 US operators used.
The results are dependent on the definition of a risk threshold for the volume of stomach of >0.8ml/kg, elsewhere in the literature 1.5ml/kg is used (compared to 0.8ml/kg in by this research group). There is limited evidence and consensus in this area.
Discussion from Journal Club Meeting (?Change of Practice)
Studies examining the reduction in pulmonary aspiration as an endpoint are essentially impossible due to the low incidence (from NAP 4, incidence 1:350,000 adult cases).
Paper adds to a growing body of evidence suggesting gastric ultrasound may be superior to fasting consensus and clinical assessment for a range of scenarios and patient populations, in this case the paediatric population.
Discussion on the challenges posed by training, image storage and governance surrounding use of point of care ultrasound to guide clinical decision making.
Summary by Dr M Addy. Journal Club Meeting 21 November 2019.
Image from http://www.usra.ca/regional-anesthesia/specific-blocks/pocus/gastric.php
